
Procalcitonin (PCT) is the propeptide of calcitonin. The production of procalcitonin during infection and sepsis does not depend on calcitonin levels, but is closely related to the release of endotoxin and inflammatory mediators in bacterial infection. Traditional biological markers, clinical symptoms, and signs lack sufficient sensitivity and specificity to guide treatment decisions for infectious diseases. As a recently applied biomarker, procalcitonin is increasingly supported by increasing evidence that detecting serum procalcitonin concentration can be used to early diagnose the type of infectious pathogen, evaluate the severity of infection, guide medication, and determine prognosis. Procalcitonin has become the most useful biomarker in the management of infection and sepsis in most parts of the world.
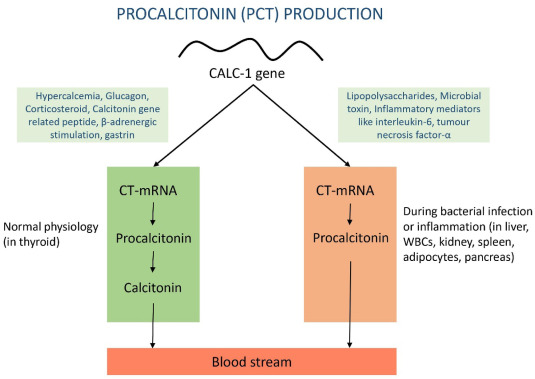
Figure 1. Specific mediators, metabolic pathways, and organs responsible for procalcitonin production in response to bacterial infections or inflammation compared to normal physiological conditions.
The diagnosis of infection has always been a major problem faced by clinicians. Although there are many monitoring methods, there is still a lack of sensitive and specific dynamic monitoring indicators. Since it was first discovered in 1993 that the concentration of procalcitonin in the blood of patients with sepsis was significantly elevated, procalcitonin has become an important marker for the diagnosis of bacterial infection. Procalcitonin has higher accuracy and specificity than traditional biological markers. At the same time, PCT concentration is related to the severity of the disease and can be used to guide antibacterial drug treatment.
Production and Release of Procalcitonin
Procalcitonin is the propeptide of calcitonin and consists of 116 amino acids. Normally procalcitonin is encoded by the Calc-1 gene located on the short arm of chromosome 11 in thyroid C cells. In thyroid C cells, the Calc-1 gene is translated into a PCT precursor peptide containing 141 amino acids, and then enters the endoplasmic reticulum to form PCT under the action of glycosylase and specific enzymes. Subsequently, PCT is processed by specific endopeptidase, cleaved into N-PCT, calcitonin and calstatin.
Under normal circumstances, PCT is almost not secreted from cells, and the blood content is <0.1ng/ml. Once bacteria invade the body, the PCT concentration in the blood can quickly increase to 5,000 times. The reason for this is that some studies believe that bacterial infection stimulates specific transcription factors in tissues to activate the Cala-1 regulatory gene, thereby activating PCT transcription. Others believe that under normal circumstances, PCT transcription is inhibited by specific transcription factors. After bacterial infection, this inhibitory factor is cleaved, resulting in PCT transcription.
Unlike C-reactive protein, almost all peripheral tissues are involved in the production of PCT during bacterial infection. Studies on thyroidectomy patients have found that blood PCT concentrations remain high during bacterial infection. Researchers injected endotoxin into baboons and found that PCT-mRNA was expressed in almost all tissues. The liver and kidney were the main tissues producing PCT 6 hours after the injection of endotoxin. About 24 hours after the injection, the lungs, stomach, the heart produces PCT at its peak. The half-life of PCT in the circulation is approximately 22 to 26 hours and does not depend on renal excretion.
It is controversial whether peripheral blood cells, in addition to parenchymal cells, participate in the production of PCT during bacterial infection. Scientists studied the peripheral blood of 17 patients with moderate to severe infections and found that PCT could be detected in monocytes and lymphocytes. By intracellular antibody staining, the researchers confirmed the expression of PCT in monocytes and neutrophils. However, the researcher believes that peripheral blood mononuclear cells cannot produce PCT even when stimulated by endotoxins and cytokines. Other investigators found that PCT-mRNA was not detected in endotoxin-stimulated macrophages or viable isolated peripheral blood mononuclear cells. Therefore, whether peripheral blood cells are involved in the release of PCT during bacterial infection still requires further study.
Current research suggests that there are two pathways for bacteria to induce the release of PCT, namely the direct and indirect pathways. In the direct pathway, bacterial tissue structures (DNA, fimbriae, peptidoglycan, etc.) directly induce intracellular signaling to release PCT. In the indirect pathway, pathogens stimulate the body to produce intermediaries (such as pro-inflammatory cytokines) that then act on target cells to produce PCT. Some researchers believe that during bacterial infection, the pathogen directly acts on the specific microorganism-related receptor at the No. 5 start site of the Calc-1 gene, causing a large amount of PCT to be released. On the contrary, another researcher found that during bacterial infection, bacterial endotoxin stimulates the body to produce a series of pro-inflammatory cytokines (such as TNFa, IL-1β, IL-8, IL-6) that stimulate tissues other than the thyroid gland (intestine, lung , immune cells) release PCT into the blood. Both clinical and animal studies have confirmed that direct injection of endotoxin results in the release of PCT in the blood. Some researchers add endotoxin to cells cultured in vitro can cause intracellular production of PCT. Intravenous injection of TNFa and IL-2 into cancer patients causes rapid and large release of PCT. Interestingly, infusion of anti-TNFa monoclonal antibodies into human leukocytes inhibited bacterial-induced stimulation of PCT release. Another study found that IFN-r inhibits the release of PCT.
Application of PCT in Infectious Diseases
Differentiate bacterial infections from non-bacterial infectious diseases
The Infectious Diseases Society of America and the American Society of Critical Care Medicine jointly recommend PCT as an auxiliary diagnostic marker to distinguish sepsis from non-infectious systemic inflammatory responses. When bacterial infection causes a systemic inflammatory reaction, PCT concentration will increase significantly. However, when viral infection, cancer fever, transplant-host rejection and other inflammatory reactions occur, the blood PCT concentration will not increase or only increase slightly.
Evaluate the degree of infection and prognosis
Blood PCT concentration is not only a specific indicator of infectious diseases, but also can monitor the severity of host infection and judge prognosis by continuously monitoring PCT levels. The concentration of PCT is related to the severity of bacterial infection and bacterial load.
Application of PCT in Infections in Special Populations
Neonatal bacterial infection is one of the most important health problems, and early diagnosis and treatment are very important due to the non-specific symptoms and signs and high mortality rate after neonatal bacterial infection. Studies found that neonates with sepsis, urinary tract infection, and meningitis had significantly higher blood PCT concentrations. Current research has confirmed the value of PCT in neonatal infections. Based on these research results, the sensitivity and specificity of PCT They were 76.9% and 100% respectively, and the positive prediction rate and negative prediction rate were 100% and 78% respectively.









